Title
题目
Improving the noninvasive classification of glioma genetic subtype with deep learning and diffusion weighted imaging
通过深度学习和弥散加权成像提高胶质瘤遗传亚型的无创分类
Background
背景
Diagnostic classification of diffuse gliomas now requires an assessment of molecular features, often
including IDH-mutation and 1p19q-codeletion status. Because genetic testing requires an invasive process, an alternative noninvasive approach is attractive, particularly if resection is not recommended. The goal of this study was to evaluate the effects of training strategy and incorporation of biologically relevant images on predicting ge netic subtypes with deep learning.
扩散性胶质瘤的诊断分类现在需要评估分子特征,通常包括IDH突变和1p19q共失状态。因为遗传测试需要一个侵入性过程,所以一个非侵入性的替代方法显得很有吸引力,特别是在不推荐切除的情况下。本研究的目标是评估训练策略和融入生物学相关图像对使用深度学习预测遗传亚型的影响。
Conclusions
结论
Training a classifier to predict both IDH-mutation and 1p19q-codeletion status outperformed a tiered
structure that first predicted IDH-mutation, then 1p19q-codeletion. Including apparent diffusion coefficient (ADC), a surrogate marker of cellularity, more accurately captured differences between subgroups.
训练一个分类器同时预测IDH突变和1p19q共删除状态的表现优于先预测IDH突变,然后预测1p19q共删除的分层结构。包括表观弥散系数(ADC),一种细胞性的代理标记,能更准确地捕捉亚组之间的差异。
Results
结果
The best model used a 3-class CNN containing diffusion-weighted imaging as an input, achieving 85.7% (95% CI: [77.1, 100]) overall test accuracy and correctly classifying 95.2%, 88.9%, 60.0% of the IDHwt, IDHmut-intact, and IDHmut-codel tumors. In general, 3-class models outperformed tiered approaches by 13.5%-17.5%, and models that included diffusion-weighted imaging were 5%-8.8% more accurate than those that used only anatomical imaging.
最佳模型采用了一个包含弥散加权成像输入的三类CNN,达到了85.7%(95% CI:[77.1, 100])的总测试准确率,并正确分类了95.2%的IDH野生型(IDHwt)、88.9%的IDH突变/未共删除(IDHmut-intact)和60.0%的IDH突变/共删除(IDHmut-codel)肿瘤。总体来说,三类模型的表现优于分层模型13.5%-17.5%,包含弥散加权成像的模型比只使用解剖成像的模型准确度高出5%-8.8%。
Method
方法
Our dataset consisted of 384 patients with newly diagnosed gliomas who underwent preoperative MRI with standard anatomical and diffusion-weighted imaging, and 147 patients from an external cohort with anatom ical imaging. Using tissue samples acquired during surgery, each glioma was classified into IDH-wildtype (IDHwt), IDH-mutant/1p19q-noncodeleted (IDHmut-intact), and IDH-mutant/1p19q-codeleted (IDHmut-codel) subgroups. After optimizing training parameters, top performing convolutional neural network (CNN) classifiers were trained, validated, and tested using combinations of anatomical and diffusion MRI with either a 3-class or tiered structure. Generalization to an external cohort was assessed using anatomical imaging models.
我们的数据集包括384名新诊断的胶质瘤患者,这些患者接受了术前MRI检查,包括标准的解剖和弥散加权成像,以及147名来自外部队列的患者,这些患者接受了解剖成像。使用在手术中获得的组织样本,每个胶质瘤被分类为IDH野生型(IDHwt)、IDH突变/1p19q未共删除(IDHmut-intact)和IDH突变/1p19q共删除(IDHmut-codel)亚组。在优化训练参数之后,使用解剖和弥散MRI的组合,训练、验证和测试表现最佳的卷积神经网络(CNN)分类器,采用三类或分层结构。使用解剖成像模型评估对外部队列的泛化能力。
Figure
图
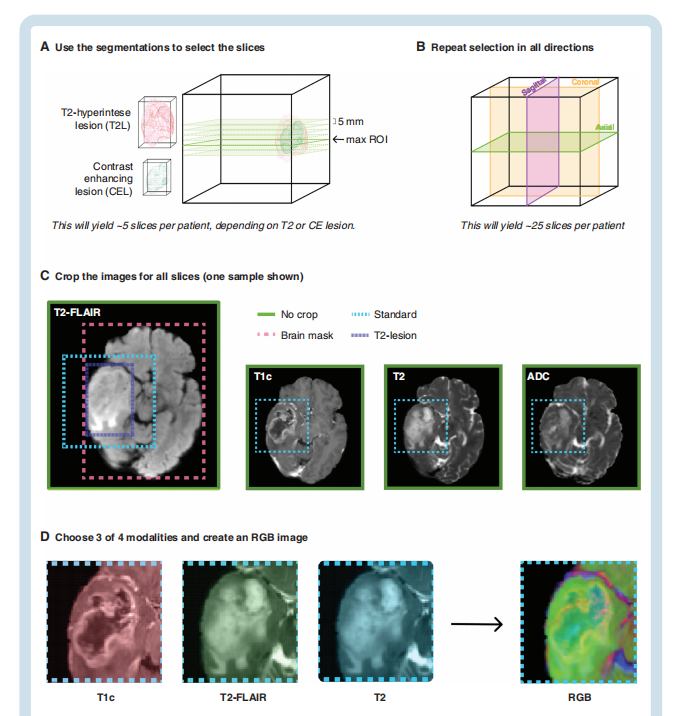
Fig. 1 Schematic of image processing strategy. (A) Segmented contrast-enhancing (CEL) or T2 (T2L) lesions were used to automatically select the slices by first selecting the central slice with maximum area and expanding every 5 mm until the boundary of the lesion was reached. (B) This process was repeated in each direction: axial, coronal, and sagittal. (C) Images were then cropped to either the brain mask, the T2L, a standard size, or were not cropped. (D) Three of the four sequences of interest (T2-FLAIR, T1c, T2, and ADC) were placed in the R, G, and B channels of a color image that was used as the input to the network.
图 1 图像处理策略示意图。(A) 使用分割的对比增强(CEL)或T2(T2L)病变自动选择切片,首先选择最大面积的中心切片,并每隔5毫米扩展直至病变边界。(B) 这一过程在每个方向上重复:轴向、冠状和矢状。(C) 然后将图像裁剪为大脑掩模、T2L、标准尺寸,或不裁剪。(D) 四个感兴趣的序列中的三个(T2-FLAIR, T1c, T2, 和 ADC)被放置在彩色图像的R、G、B通道中,这个彩色图像被用作网络的输入。
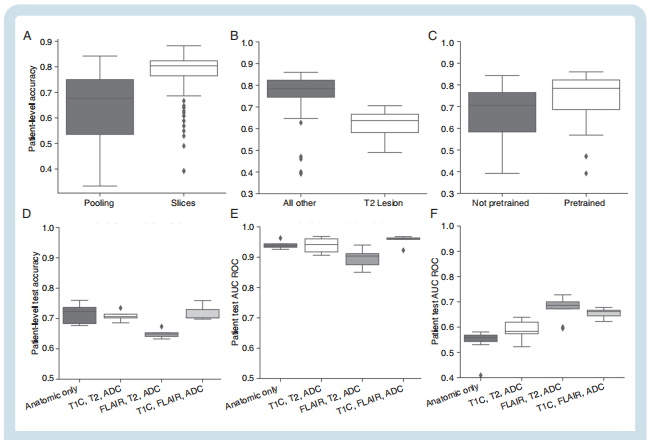
Fig. 2 Main insights from the hyperparameter search and effects of including ADC as an input image. (A–C) Hyperparameter search: (A) A slice by-slice prediction approach improved the ability to achieve high accuracy on the validation data compared to average pooling of slices. (B) Cropping to the T2-lesion reduced the validation accuracy of the 3-class model. (C) Pre-training increased validation accuracy of the model. (D–F) Benefit of including ADC as an input image: (D) For the 3-class models, lower generalization accuracy was observed when ADC replaced T1c, while replacing the T2 image with ADC achieved the best performance. (E) For the IDH-mutation tier, test accuracy was slightly improved using T1c, T2-FLAIR, and ADC as input images. (F) For the 1p19q mutation tier, replacing T1c with ADC significantly improved test accuracy.
图 2 超参数搜索的主要见解及包括ADC作为输入图像的效果。(A-C) 超参数搜索:(A) 逐切片预测方法相较于切片的平均汇集,提高了在验证数据上达到高准确率的能力。(B) 裁剪至T2病变降低了三类模型的验证准确率。(C) 预训练提高了模型的验证准确率。(D-F) 包括ADC作为输入图像的好处:(D) 对于三类模型,当ADC替换T1c时,观察到较低的泛化准确率,而用ADC替换T2图像则获得了最佳表现。(E) 对于IDH突变层,使用T1c、T2-FLAIR和ADC作为输入图像略微提高了测试准确率。(F) 对于1p19q突变层,用ADC替换T1c显著提高了测试准确率。
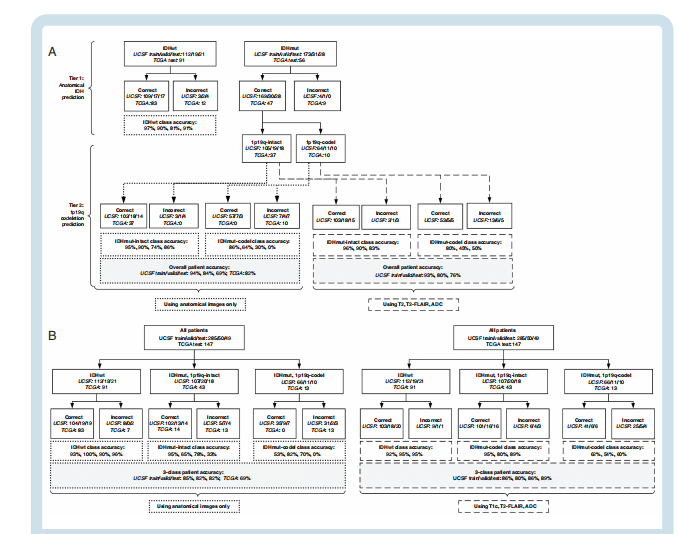
Fig. 3 Final patient accuracy and class accuracies of the final four models: (A) A 2-tiered structure with all anatomical images (left) and ADC replacing the T1c image in the second tier (right). (B) A 3-class structure with anatomical images only (left) and ADC replacing T2 as the third channel (right). An increase in the IDHmut-codel accuracy and overall accuracy was observed when ADC maps were included as input images. The best model was the 3-class model that included ADC.
图 3 最终四个模型的患者准确率和类别准确率:(A) 一个两层结构,包含所有解剖图像(左)和在第二层中用ADC替换T1c图像(右)。(B) 一个仅包含解剖图像的三类结构(左)和用ADC替换T2作为第三通道(右)。当将ADC图作为输入图像包括在内时,观察到IDHmut-codel准确率和总体准确率的提升。最佳模型是包括ADC的三类模型。
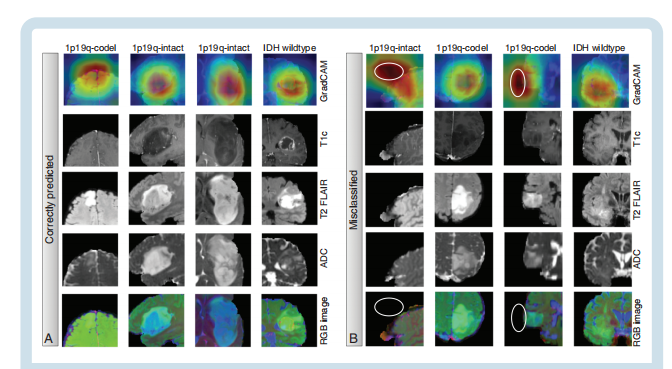
Fig. 4 Visualization of imaging features and GradCAM analysis of the best (A) and worst (B) predicted patients with the final 3-class model that included ADC. GradCAM maps of the worst predicted patients often indicated that these models were looking outside of the tumor region when making their decision (white ellipses), compared to looking at the lesion for all of the correctly predicted patients. Top column lists true groupings. IDHwt and IDHmut-intact were misclassified as IDHmut-codel gliomas, while the IDHmut-codel examples were predicted as IDHmut-intact.
图 4 最佳(A)和最差(B)预测患者的影像特征和GradCAM分析,使用的是包含ADC的最终三类模型。对最差预测患者的GradCAM图通常表明,这些模型在做出决定时常常观察肿瘤区域之外(白色椭圆),与所有正确预测的患者观察病变区域相比。顶部列出了真实分组。IDHwt和IDHmut-intact被误分类为IDHmut-codel胶质瘤,而IDHmut-codel的例子被预测为IDHmut-intact。
Table
表
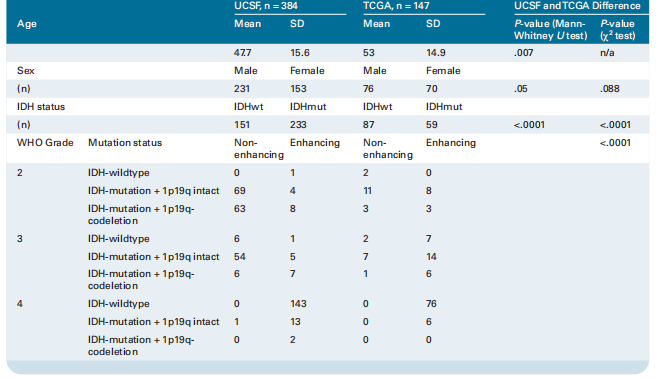
Table 1. Clinical and Demographic Characteristics of the Patient Population Included in This Study
表 1. 本研究包括的患者人群的临床和人口统计特征
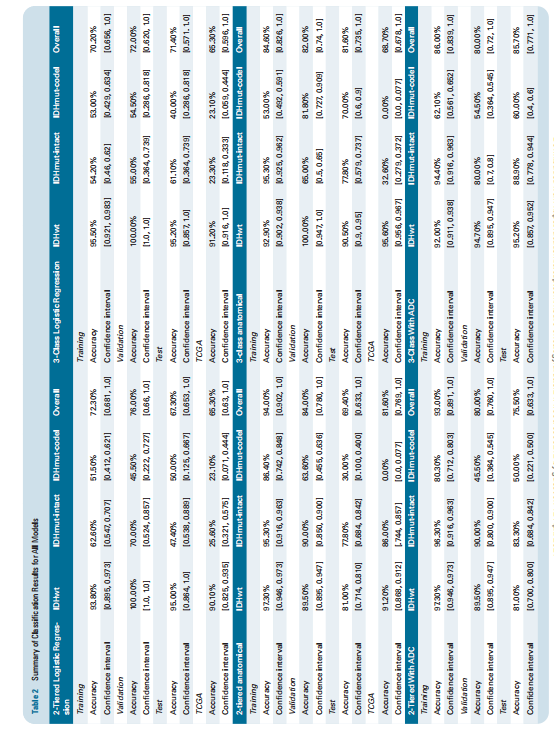
Table 2 Summary of Classification Results for All Models
表 2 所有模型的分类结果摘要